2410
WHO has recognized obesity as a global problem that amounts to an epidemic. This is especially true among children; in some countries their number reaches 25%. At the same time, exogenous constitutional obesity is a rather dangerous pathology, which is characterized by a profound violation of the fermentation and metabolic systems.
This leads to an imbalance between fat production and low energy expenditure. Doctors consider this pathology as a complex disease, which has a typical clinical picture.
Characteristics and description of pathology
Constitutional exogenous obesity is a hereditary disease caused by the intake of large amounts of calories from food and fat deposition as a result of genetic predisposition. This disease responds well to treatment because it is not associated with a disruption of the hormonal system.
With such obesity, fat deposits can reach up to 70% of a person’s total weight. Typically, fat accumulates on the chest, hips, pelvis, and abdomen. If obesity is severe, then differences between body parts disappear.
Exogenous constitutional obesity can provoke a disorder of the hormonal system, but is not caused by disturbances in it. This disease affects many older people today. It depends on a person’s diet, so it is often diagnosed in those who consume large quantities of food containing carbohydrates and fats, but at the same time spend little energy.
The main danger of such obesity is the deposition of fat around the internal organs, as well as in the fiber that is located under the skin . This can lead to deterioration in the functioning of organs and systems and the emergence of many health problems.
Exogenous obesity is diagnosed in 75% of people worldwide who consume high-calorie foods. This phenomenon is relevant in early childhood, adolescence, during pregnancy, menopause in women, and adulthood in men.
Children and adolescents with obesity today make up a significant portion of all patients observed by both pediatric endocrinologists and registered with pediatricians.
This is due to both the general trend towards an increase in obesity in pediatric practice, observed everywhere, and the more active detection of this condition - based on the results of “returning” dispensary examinations and regular outpatient appointments - based on the general anxious mood of doctors, confirmed by the results of international long-term prospective observations. It is known that obese children and adolescents, unlike their thin peers, have more health problems and are more likely to be obese in adulthood. Obesity, which begins in childhood, is a risk factor for type 2 diabetes mellitus, arterial hypertension, atherosclerosis, apnea syndrome, cardiovascular accidents - myocardial infarction and stroke, coronary heart disease, non-alcoholic fatty liver disease, some types of tumors, musculoskeletal diseases - motor system. No less important is the eating disorder associated with the development of obesity, which in adolescence can acquire the features of independent mental disorders - from bulimia and overeating with episodes of starvation to severe depression and low self-esteem, requiring observation and treatment by psychologists and psychiatrists. Unfortunately, these alarming patterns are being observed all over the world.
At the same time, like any multifactorial disease with complex etiopathogenesis, childhood obesity is difficult to systematize and classify.
It is no coincidence that today throughout the world there is no single harmonious classification that would allow identifying individual forms of obesity according to etiopathogenesis with simultaneous stratification according to metabolic, cardiovascular and other risks.
Even historically, approaches to the classification of obesity in both adults and children have been different. For example, the classification proposed by J. Mayer in 1957 took into account only the etiological factor in the development of obesity and identified 4 groups of diseases: genetically determined, hypothalamic, endocrine and drug-induced [1].
N.V. Dudenko [2] proposed to distinguish only 2 forms of obesity in children: nutritional-constitutional, associated with excess calorie consumption, and neuroendocrine (hypothalamic), which developed as a result of a toxic, traumatic or dystrophic process in the interstitial brain. At the same time, the author noted that it is with the neuroendocrine form that complaints of a neurasthenic nature, thirst, disorders of sexual development, and skin changes (striae, acanthosis, folliculitis, hypertrichosis) prevail in children. However, this classification did not take root in clinical practice, since the described symptoms occurred with equal frequency in both groups.
One of the most detailed is the classification proposed in 1985 by L.B. Silence [3], which took into account 3 components of obesity.
1. Etiological:
- dysfunction of the hypothalamus (tumors, inflammation, trauma or damage during surgery, increased intracranial pressure, functional changes);
- endocrine disorders (excess glucocorticoids, hypothyroidism, hypopituitarism, hypogonadism, hyperinsulinism);
— genetic factors (congenital predisposition to obesity and genetic syndromes associated with obesity);
— nutritional factors (mother’s nutritional factors and type of child feeding);
- medications (phenothiazines, insulin, corticosteroids, tricyclic antidepressants).
2. Morphological:
— hypercellular-hypertrophic obesity (onset at an early age, severe degree);
— pertrophic obesity (late onset, less pronounced).
3. According to pathogenesis factors: family influences, physical inactivity, dietary factors, socio-economic influence, education, cultural and ethnic factors, psychological.
Such a detailed classification reflected the developmental mechanisms known at that time, but did not take into account the degree of obesity and was mainly etiopathogenetic.
For a long time, one of the most popular in our country was the classification of Yu.A. Knyazev [4], which highlighted:
1. Clinical and pathogenetic form:
— primary (constitutional-exogenous and nutritional obesity);
- secondary (cerebral, diencephalic, endocrine);
- mixed;
- rare forms.
2. According to the degree of obesity - depending on the percentage of excess of the patient’s body weight, comparable to the “ideal” one, - I degree (15-25%), II (25-50%), III (50-100%), IV (more than 100%).
3. Course: rapidly progressing, slowly progressing, stable, regressing.
4. Complications: secondary diencephalic syndrome, dysfunction of the musculoskeletal system, cardiovascular disorders, dysfunction of the gonads, metabolic forms.
The undoubted advantage of this classification is the clinical characteristics of obesity, which is necessary for practical healthcare no less than an understanding of the etiology and pathogenesis. However, even at the current level of our knowledge, the identification of “primary” and “secondary” forms is difficult, and the course of the disease does not always reflect metabolic changes.
Subsequently, a number of authors (A.I. Kliorin, M.A. Zhukovsky, N.T. Starkova) proposed their own classifications, which were variants of a more detailed, improved classification by Yu.A. Knyazeva [5].
At the same time, other researchers - D.Ya. Shurygin (1980), E.A. Beul (1986) did not differentiate different forms of obesity from the point of view of etiopathogenesis. In particular, studies by D.Ya. Shurygina et al. [6], using the example of simple obesity and obesity in patients with Prader-Willi syndrome, showed that this condition, regardless of some features of etiology and pathogenesis, becomes to a certain extent a uniform “clinical phenomenon.”
No less interesting is the absence of any classification of obesity in children in most modern foreign guidelines - T.R. Harrison (2005), C. Brook (2008), American Endocrine Society Consensus on Obesity in Children and Adolescents (2008).
This once again emphasizes the difficulty of creating a unified classification of a multifactorial disease.
At the same time, I would like the classification to help the doctor in daily practice - and not only from a clinical point of view, but also correspond to the legal environment in which communication between the doctor and the patient takes place today - in the general health insurance system, based on the implementation of each nosological a unit of certain medical standards, the diagnoses of which must correspond to the codes of the International Classification of Diseases, 10th revision (ICD-10).
Thus, having realized the “scale” of the problem, gained historical experience, and also armed with new knowledge and modern working conditions for a doctor in practical healthcare, we propose a new version of classification for children and adolescents.
1. By etiology:
- simple (constitutional-exogenous, idiopathic);
- hypothalamic;
— obesity in neuroendocrine diseases (hypercortisolism, hypothyroidism, etc.);
- iatrogenic obesity (caused by long-term use of glucocorticoids, antidepressants and other drugs);
— monogenic obesity;
- syndromic obesity.
2.
Based on the presence of complications and comorbid conditions
:
— disorders of carbohydrate metabolism (impaired glucose tolerance, impaired fasting glycemia, insulin resistance);
- non-alcoholic fatty liver disease (fatty hepatosis and steatohepatitis as the most common conditions in children);
- dyslipidemia;
- arterial hypertension;
— diabetes mellitus type 2;
- delayed sexual development (and relative androgen deficiency);
- accelerated sexual development;
- gynecomastia;
- hyperandrogenism syndrome;
- apnea syndrome;
- disorders of the musculoskeletal system (Blount's disease, osteoarthritis, spondylolisthesis, etc.);
- cholelithiasis.
3.
According to the degree of obesity:
- SDS BMI 2.0-2.5 - I degree;
— SDS BMI 2.6—3.0 — II degree;
— SDS BMI 3.1—3.9 — III degree;
— SDS BMI ≥4.0 — morbid.
Note.
The criteria for overweight and obesity in children are determined according to percentile tables or standard deviation scores (SDS - standard deviation score) of the body mass index (BMI). They take into account not only height and body weight, but also the gender and age of the child. Taking into account WHO recommendations, we propose to define obesity in children and adolescents as +2.0 SDS BMI, and overweight from +1.0 to +2.0 SDS BMI.
An example of a diagnosis formulation taking into account the ICD code
ICD codes:
— (E 66.0) Obesity caused by excess supply of energy resources;
— (E 66.1) Drug-induced obesity;
— (E 66.2) Extreme obesity, accompanied by alveolar hypoventilation;
— (E 66.8) Other forms of obesity;
— (E 66.9) Obesity, unspecified;
— (E 67) Other types of excess nutrition;
— (E 67.8) Other specified forms of nutritional excess;
— (E 68) Consequences of excess nutrition.
Examples:
— (E 66.0) Constitutional-exogenous obesity of the third degree (SDS BMI = 3.26). Dyslipidemia. Impaired glucose tolerance.
— (E 89.3) Craniopharyngioma, condition after removal. Hypothalamic morbid obesity (SDS BMI=4.2). Hypopituitarism.
— (E 66.8) Monogenic obesity caused by proopiomelanocortin deficiency (SDS BMI=2.8). Secondary adrenal insufficiency.
(E 67.8) Prader-Willi syndrome: stage III obesity (SDS BMI = 3.7), delayed psychomotor development. Condition after orchidopexy (05.2013). Dyslipidemia.
Several comments on each classification point.
1. By etiology
We propose to distinguish 5 obesity groups.
Simple (constitutional-exogenous, idiopathic) - obesity associated with excess calorie intake in conditions of physical inactivity and hereditary predisposition.
This is the largest group, accounting for up to 98-99% of all cases of obesity.
The onset of the disease most often occurs after the age of 5 years, or at the beginning of puberty. As a rule, obesity is of a gradually progressive nature, against the background of good (often accelerated) growth rates. Marked weight gain during puberty. The presence of striae, follicular keratosis, polyphagia, acanthosis, arterial hypertension, etc. does not always correlate with the degree of obesity. It is typical to have overweight and obesity in relatives (parents, grandparents), and therefore this form is often called “constitutional.” What is the contribution of genetics to the development of this type of overweight?
Obesity is a multifactorial disease that results from a specific interaction of genetic and non-genetic causes. The role of “heredity” in the development of obesity is proven by the different incidence of this disease in different ethnic groups and the higher concordance in the development of pathology in identical twins. Thus, recent family studies, as well as work on twins, have shown that from 40 to 70% of changes in body mass index (BMI) can be explained by genetic factors [7].
Thus, simple obesity is a polygenic disease. Recent publications have described more than 430 genes, markers and chromosomal regions associated with obesity in humans.
However, according to modern concepts, the contribution of each gene to the predisposition to obesity is relatively small.
Since 2005, the world began to use the method of genomic association analysis to study multifactorial diseases, based on the identification of polymorphic mononucleotide substitutions, or SNPs - single nucleotide gene polymorphisms, uniformly covering the entire human genome. The use of this method makes it possible to scan the entire human genome for the presence of genetic markers of susceptibility to any multifactorial disease using numerous samples of sick and healthy individuals. In general, this makes it possible to identify significant genetic risk markers, whose contribution to the genetic predisposition to a particular disease is relatively small.
To date, genomic association analysis has identified about 32 chromosomal regions associated with the development of obesity. Among them are regions near the melanocortin type 4 receptor gene ( MC4R
) and the gene associated with the development of fat mass and obesity (
FTO)
. It has been shown that the weight of most carriers of these alleles exceeds the weight of the control group by no more than 500 g [8].
The largest study to date to study the genetic influence on BMI (Genetic Investigation of Anthropometric Traits - GIANT), based on genomic association analysis, included more than 123 thousand Europeans and found that each of the risk alleles contributes to an increase in BMI by 0.17 kg/m2. However, the total alleles of all known 32 chromosome segments explain only 1.5% of the total BMI variability [9].
In addition, comparative analysis of the study results separately for children and adults showed extensive overlap of risk alleles for overweight and obesity in all groups, so that to date there is no molecular genetic explanation for early and late onset of obesity. In addition, the identified risk alleles are practically the same between adolescents of European and East Asian origin [8].
All this once again confirms the immutability of the genetic component, which does not explain the pronounced increase in obesity throughout the world over the past 30 years.
Modern studies of the characteristics of the quantitative and qualitative development of adipose tissue itself, both brown and white, and the active substances and hormones secreted by it look promising.
Thus, despite the fact that obesity is a disease with a hereditary predisposition, the likelihood of its development and the degree of manifestation largely depend on lifestyle and diet.
Hypothalamic
- obesity associated with the presence and treatment of tumors of the hypothalamus and brain stem, radiation therapy for brain tumors and hematological malignancies, skull trauma or stroke.
Hypothalamic obesity is a serious complication that occurs in 30-70% of children who have undergone surgery or radiation treatment for tumors of the hypothalamus and brain stem, as well as skull trauma.
Damage to the ventromedial hypothalamus is believed to be involved in the pathogenesis of this form of obesity, supported by studies in animal models.
As a rule, in most cases, obesity of a rapidly progressive nature develops after surgery (radiation therapy); less often, it precedes the period of diagnosis. In the case of craniopharyngioma, most patients experience slow growth; for gliomas - symptoms of premature sexual development; neurological complaints (headache, blurred vision) depend on the location and progression of the tumor.
Speaking of metabolic characteristics, according to our center, patients with hypothalamic obesity have comparable values of insulin, insulin resistance and leptin with the group of simple obesity. However, these patients have severe dyslipidemia, as well as lower growth and insulin-like growth factor 1 [10].
Unfortunately, to date, any dietary or pharmacological interventions for this form of obesity are ineffective. The best way to treat hypothalamic obesity is its prevention, based on improving surgical treatment methods, adherence to the regimen and principles of rational nutrition in the postoperative period [11].
Obesity in neuroendocrine diseases
(hypercorticism, hypothyroidism, hypopituitarism, etc.).
This form of obesity is always secondary to the underlying disease, depends on the time of its debut and is stopped with effective treatment of the underlying disease - the prescription of growth hormone for somatotropic insufficiency, levothyroxine for hypothyroidism, effective therapy for hypercortisolism.
Obesity is iatrogenic
- caused by long-term use of glucocorticoids, antidepressants and other drugs. A more frequent phenomenon in modern conditions, associated with the increased use of a number of antidepressants. The peculiarity of this form is that, unlike the previous one, even after stopping therapy, which caused an increase in appetite as a side effect and led to a gain of excess body weight, the habit of “eating” remains, and then obesity develops according to its own laws, regardless of the initial disease . The situation is aggravated by long-term treatment of the underlying disease. A method of prevention is to explain to the patient (his parents) the possible side effects of therapy, to prevent the development of excess body weight by maintaining a balanced, normal calorie diet.
Monogenic obesity
- obesity that develops as a result of mutations in single genes. To date, 8 forms have been described that are caused by mutations in the genes of the “leptin-melanocortin pathway” - leptin, leptin receptor, melanocortin receptors types 3 and 4, proopiomelanocortin, proconvertase type 1, neurotrophic factor receptor - tropomyosin-related kinase B, a transcription factor involved in the development and functioning of the ventromedial nuclei of the hypothalamus - single-minded 1 [12-14]. Morbid obesity, progressing from the first months of life against the background of severe polyphagia, is the most common feature of all monogenic forms, confirming the central role of these genes in the regulation of body weight.
These are the rarest forms of obesity, the total number of patients reaches tens of people. Most patients with proven mutations are children from consanguineous marriages. The only country in the world in which 20% of severe obesity is due to monogenic forms is Pakistan, which is also explained by the high frequency of consanguineous marriages [15]. Linear growth and mental development of patients are not affected. Children with congenital deficiency of leptin and melanocortins are characterized by early severe hyperinsulinemia, accompanied by the development of type 2 diabetes mellitus, often in the 3rd–4th decade of life [12]. The combination of rapidly progressive morbid obesity, increased appetite and adrenal insufficiency with undetectable serum levels of cortisol and ACTH is characteristic of congenital proopiomelanocortin deficiency [13]. Early severe obesity, hypogonadotropic hypogonadism, postprandial hypoglycemia, low serum cortisol levels in combination with malabsorption syndrome are typical for type 1 convertase deficiency [14].
An effective treatment is subcutaneous administration of recombinant human leptin, possibly only in cases of leptin deficiency.
Syndromic obesity
- obesity observed in chromosomal and other genetic syndromes - Prader-Willi, Ahlström, Cohen, Down, Lawrence-Moon-Bardet-Biedl, pseudohypoparathyroidism, fragile X chromosome, etc. These forms of obesity are characterized by wide clinical polymorphism. Features of syndromic forms of obesity are different ages of onset of obesity - from the first months of life to late childhood, different degrees of its severity - from moderate to morbid, and the presence of specific phenotypic features. As a rule, all these patients have neurological disorders, severe delayed psychomotor development and reduced intelligence.
Although genetic defects and markers have been identified for most syndromes, their function remains unknown. Therefore, the pathogenesis and causes of the development of obesity syndromic forms have also not been established.
At the same time, early diagnosis of syndromic forms is important - both for early screening of severe comorbid conditions and their timely treatment (retinal pathology in Alström syndrome, hypocalcemia and diabetes mellitus in pseudohypoparathyroidism, fatal apnea in Prader-Willi syndrome), and for preventing the development of morbid obesity .
Thus, with Prader-Willi syndrome, children have moderate weight gain during the 1st year of life against the background of severe muscle hypotonia. And as hypotension decreases by the 2-3rd year of life, polyphagia joins in, followed by the rapid development of morbid obesity. The mechanisms of increased appetite in this form are not fully understood. However, international experience emphasizes the importance of timely training of parents in the principles of rational nutrition to prevent “overfeeding” of a child with Prader-Willi syndrome in the 2nd year of life as a real way to prevent obesity.
2.
According to the presence of complications and comorbid (associated) conditions
Our analysis on the example of 730 obese children and adolescents who applied to the Research Institute of Pediatric Endocrinology of the Federal State Budgetary Institution Scientific Center in 2008-2013 showed that the most common metabolic disorders are dyslipidemia, various disorders of carbohydrate metabolism (impaired glucose tolerance, insulin resistance, impaired fasting glycemia), while lesions of other systems are detected less frequently: fatty hepatosis, steatohepatitis, delayed puberty, hyperandrogenism syndrome, arterial hypertension, etc. The specificity of the study of disorders in obesity according to the data of referrals will vary: for cardiologists it will be arterial hypertension, for andrologists - delayed sexual development. This is due to both the general underestimation of obesity by parents and, as a rule, late referral to doctors of the appropriate profile depending on the leading complaint, and the lack of a unified state system for the active identification and monitoring of children and adolescents with obesity. Simply put, a parent will actively come to an appointment with their teenage child to a cardiologist with complaints of increased blood pressure or to a gynecologist with complaints of the lack of a regular menstrual cycle, and not to a pediatrician and endocrinologist 5-10 years earlier with complaints of excess body weight. But at the same time, comparing our data with international ones, it should be noted that the results are comparable—more and earlier detection of metabolic disorders than other comorbid conditions, and therefore we propose to evaluate them in more detail. Data from international studies demonstrate that early detection of such changes and their timely correction is the key to successful prevention of obesity-associated diseases in adulthood.
3. And finally, an equally controversial criterion in the classification is the determination of the degree of obesity.
It should be noted that today in most countries of the world there are no degrees of obesity in children and adolescents. This is due to work including studies from our center [10], which demonstrated that the degree of obesity does not always determine the presence or absence of metabolic and other disorders. Children with slight excess body weight may have various complications, while patients with morbid obesity may have normal levels of carbohydrate and fat metabolism, the absence of fatty hepatosis and other disorders. To be fair, it should be noted that in most domestic works by cardiologists there is a clear relationship between the degree of obesity and blood pressure.
In general, in our country, obesity has traditionally always been classified into degrees depending on excess body weight. Most doctors are accustomed to this principle. In addition, when communicating with parents of obese children, an important psychological aspect of this approach should be noted: the awareness that your child is “already in the second or third degree of obesity” is often the only argument that makes adults think about the “development prospects” of the little person and, as a consequence, — start helping him achieve a healthy lifestyle trajectory.
Anticipating the inevitable critical assessment of the proposed classification, I would like to emphasize that this version of the classification is the first step in the formation of a common language that would be understandable and convenient for both pediatricians and endocrinologists, as well as all doctors involved in the observation of such patients - gastroenterologists , cardiologists, gynecologists.
The authors declare that there is no conflict
of interest related to the data presented in the article.
Types of obesity
In medicine, obesity is conventionally divided into two types:
- The female type or gynodal is characterized by the deposition of fat in the abdomen, thighs and buttocks. This figure resembles a pear in shape. The disease has a favorable prognosis, as it responds well to therapy and does not pose a threat to health. This distribution of fat deposits is associated with an increase in the concentration of estrogen; it is usually located in the fiber that is located under the skin.
- The male or android type is characterized by the deposition of fat in the chest, abdomen and shoulders, as well as around the abdominal organs. Such obesity can threaten health, as it often causes metabolic and hormonal system disorders. The pathology must be promptly eliminated, as there is a risk of developing dangerous diseases that require medical and surgical treatment.
According to statistics, obesity provokes the development of heart defects, which leads to death or disability.
General information about exogenous constitutional obesity
Alimentary or primary – these are the names for the type of obesity that is caused by non-hormonal reasons. The exogenous constitutional form of the disease is characterized by a significant increase in the amount of adipose tissue. This occurs as a result of an imbalance between the energy supplied by food and its expenditure. The pathology is distinguished by its progressive nature. Endocrinologists distinguish several degrees of the disease, which have their own characteristics:
Body fat, % of body weight
Excess weight from normal, %
Degree of disease development
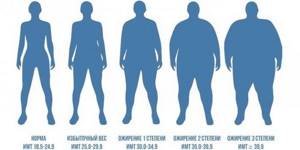
In medicine, there are four stages (degrees) of disease development:
- Exogenous-constitutional obesity of the 1st degree is characterized by an increase in a person’s weight from fifteen to twenty-nine percent of the initial body weight. At the same time, a person usually feels well, has no health problems, and lives a full life.
- Exogenous-constitutional obesity of the 2nd degree is caused by an increase in weight from thirty to forty percent of the initial body weight. During this period, a person feels weak, drowsy, and often finds it difficult to breathe.
- Obesity of the third degree, in which body weight increases from forty to fifty percent. It is difficult for a person to perform power loads, and symptoms increase.
- The last fourth degree of pathology is caused by excess body weight by more than fifty percent. This condition becomes dangerous to health and life, as internal organs begin to suffer and the person cannot move. This stage of the disease is rarely diagnosed because people usually do not live to see it.
Be sure to read: Doctors' advice on how to lose weight after 50 years for a woman with menopause
At the second and third stages of pathology, disturbances of the endocrine system and metabolic processes appear. The risk of developing a stroke or heart attack, arthrosis, arthritis, and problems with the spinal column increases. During the third stage, swelling develops, a disorder of fat metabolism occurs, and pathologies of the cardiovascular system develop.
What is stage 2 obesity?
The clinical manifestation of excess weight is called obesity.
When body weight exceeds the indicators by 30% or more, this is the 2nd degree of pathology. The norm can be determined using the BMI (body mass index) formula: weight (kg) divided by height (m) squared. Normal values are from 18.5 to 25 kg/m2. The prevalence of stage 2 obesity in women is twice as high as in men.
The dangers of being overweight
Excess fat causes many dangerous complications. List of possible consequences of second degree obesity:
- pancreatitis;
- haemorrhoids;
- cholelithiasis;
- fatty hepatosis;
- diabetes;
- arterial hypertension;
- myocardial infarction;
- diseases of the musculoskeletal system (osteoarthrosis, scoliosis and others);
- varicose veins of the lower extremities;
- thrombus formation in blood vessels;
- pulmonary hypoventilation syndrome.

Causes of obesity
There are two main reasons for the development of pathology of this form:
- Genetic predisposition;
- Eating high-calorie foods with low levels of physical activity.
With constant overeating, consumption of fatty and high-carbon foods, inactive lifestyle, combined with hereditary predisposition, exogenous constitutional obesity develops. Typically, this problem is observed in families that have a developed so-called cult of food; all family members eat unbalanced and unhealthy food.
Factors that influence weight gain are frequent stress and depression, this is especially true in women. This type of disease is constantly progressing and therefore requires timely treatment.
Obesity is exogenous - constitutional treatment
Obesity is exogenous - constitutional treatment requires an individual approach, depending on the patient’s stage of obesity. At the Rehab Family clinic, our specialists use a combined approach to the treatment of exogenous constitutional obesity, consisting of psychotherapy and physiotherapy. To help a patient cope with obesity, it is also necessary to understand him psychologically and help him cope with overeating (if any), teach him to eat properly, and in case of stressful situations, make sure that he does not have the desire to overeat. Since the problem of obesity lies in frequent overeating and accumulation of fats in the body, and with exogenous constitutional obesity this is the case, then a significant role in treatment will be assigned to working with a psychotherapist or psychiatrist. From a medication point of view, the patient will also be prescribed modern medications and an individual regimen for their administration will be developed. Our doctors will provide all the necessary assistance in curing the patient of obesity, but the patient also requires minimal participation, which consists of following medical recommendations.
Symptoms and signs of the disease
At the initial stage of development of the pathology, symptoms may not appear or be mild. If a person experiences weight gain, it is necessary to reconsider their diet. As the pathology moves into the second stage, health problems are observed. The pathology begins to progress, the weight grows rapidly. Over time, the following symptoms appear:
- Disorder of the functionality of the endocrine system;
- Development of hypertension, angina pectoris;
- Impaired kidney and liver function;
- Decreased immunity, the addition of infectious diseases.
As the disease progresses, disorders of the gastrointestinal tract, sexual function, and respiratory failure develop. A person begins to sweat a lot, which causes the development of skin diseases, for example, eczema, acne. Women may experience polycystic ovary syndrome, the development of a tumor process in the mammary gland or uterus.
A person feels headaches, weakness, fatigue after minor physical activity, aching pain in the heart, dizziness, and shortness of breath. Then joint pain appears, and arthrosis or arthritis may develop. Then mental problems, eating disorders appear, people constantly feel hungry, which is accompanied by tremors of the limbs, hypoglycemia. The appearance changes, the bangs are no longer able to lead their usual lifestyle.
Be sure to read: Strict calculation of calories consumed - AD diet
Complications and consequences
Obesity without proper treatment can provoke serious complications, as it negatively affects all systems and organs of the body.
First of all, the functionality of the heart and blood vessels is impaired, atherosclerosis and hypertension develop. This can lead to ischemia or heart attack, stroke. The respiratory system is also affected, and a person may develop pneumonia and oxygen deficiency. As the pathology progresses, the size of the stomach increases, gastritis, flatulence, and fatty degeneration develop.
Then liver diseases, cholelithiasis appear, and an intervertebral hernia develops. The risk of circulatory disorders in the brain and menstrual cycle increases significantly, and sexual development in children is delayed.
Obesity often causes diabetes mellitus, so many doctors consider this pathology as a prediabetic condition.
Diagnostic measures
Diagnosis and treatment of pathology is carried out by endocrinologists and nutritionists. First, doctors must find out the cause of the disease. To do this, they study the patient’s family history and nutrition. Typically, this form of the disease also occurs in close relatives, so establishing a diagnosis is not difficult.
Additional examinations may include:
- Tests for the concentration of thyroid and pituitary hormones;
- Study of sugar levels in the body.
Based on the examination, a final diagnosis is made and a course of treatment is developed.
Therapy
Timely treatment significantly reduces the risk of developing secondary pathologies in the body. At the initial stage of the disease, doctors prescribe a diet. High-carbohydrate and high-calorie foods should not be consumed. It is necessary to regularly engage in physical activity, perhaps using alternative medicine.
In the second degree of obesity, the diet will be more strict, physical activity should be increased. Plants that are rich in fiber and give a satiating effect, for example, flax seeds, are used as traditional medicine. The doctor also prescribes diuretics. If the disease is difficult to treat, the doctor prescribes medications aimed at suppressing appetite and removing excess fluid from the body.
At the third stage of development, you cannot do without medications. In addition, the patient adheres to a diet and exercises.
At the last stage of pathology, a surgical method of therapy is used:
- Liposuction, which is the removal of fat using a vacuum.
- Gastroplasty, in which the stomach is divided into two vertical parts. When the upper part is filled with food, the body becomes saturated.
- Abdominoplasty, in which a large sagging belly is removed.
- Enteroanastomosis, in which part of the small intestine is removed from digestion.
- Bypass surgery is the removal of part of the stomach. The amount of food a person eats becomes small. But at the same time, the patient will have to take vitamin and mineral complexes throughout his life.
- The use of gastric rings, which reduce the volume of the organ and promote rapid saturation.
- Medications that the patient also takes for life due to the onset of disability.
Be sure to read: Daily menu and principles of constructing a children's diet in a diet for weight loss
Diet is the main method of therapy
Doctors develop a diet for each patient. It includes:
- Frequent meals in small quantities, each time lowering the calorie content of the dishes.
- Chewing food slowly.
- Most meals should be consumed before lunch; the last meal should not be before bedtime, but three hours before it.
- All products should have a small amount of carbohydrates; sweets and flour dishes, and animal fats are excluded from the diet.
- Most of the food should be protein.
- The diet includes foods that have a high percentage of fiber.
- Salt and liquid should be reduced several times.
- It is unacceptable to visit fast food establishments, consume fast foods and sweet carbonated water.
In addition, a person must perform physical exercises, you can go in for sports, use physical labor.
Drug therapy
In some cases, the doctor prescribes medications that reduce appetite, normalize metabolic processes, and promote the absorption of calories. Medicines are prescribed in severe and advanced cases when conservative treatment does not bring results.
Any drug should be prescribed strictly by a doctor, since they all have side effects:
- Medicines that suppress appetite: catecholamines, cannabinoid receptor blockers.
- Drugs that enhance metabolism.
- Medicines whose action is aimed at absorbing nutrients from food, for example, Xenical or Orsoten. They interfere with the absorption of fats.
- Anorexics that suppress appetite.
For example, a doctor may prescribe one of the following medications:
- Orlistat blocks the absorption of fats in the intestines. Previously, it was produced strictly according to a prescription, but today it is freely available. Side effects include diarrhea with fatty stools. In this case, it is recommended to reduce the amount of foods that contain fat.
- "Sibutramine" is an antidepressant, anorexic, and regulates appetite. It has a number of side effects that may go away after the body adapts to the drug.
- Rimonabate is a cannabinoid receptor blocker that reduces appetite. The drug helps reduce body weight and eliminate the effects of obesity.
Obesity 2 degrees in children
According to statistics, this diagnosis occurs among all obese children in 68%. The pathogenesis of the pathology is one - hyperinsulinism. When a large amount of food enters a child's body, insulin production increases. Under its influence, hypoglycemia develops, which causes a strong feeling of hunger.
Due to constant food consumption, excess energy accumulates in adipose tissue cells. This process provokes the deposition of extra pounds. To prescribe effective treatment, the doctor finds out the reason for the accumulation of fat mass in the child.
This often occurs due to early introduction of complementary foods or overfeeding the baby with formula milk.
In older age, metabolic disorders often arise due to a psycho-emotional factor: an unfriendly atmosphere at school or family, disagreement with peers. In this case, the work of a psychologist is important. Stage 2 obesity can often be managed with diet and sports activities. Drug therapy is prescribed to a child in advanced cases with a high risk of complications.
Preventive actions
Obesity is a serious illness that can lead to disability and even death. Therefore, it is important to control your body weight; if you gain extra pounds, you need to pay attention to your diet. The risk group includes the following categories of people:
- People whose relatives were obese;
- Adults who do not move much;
- Young people with a high appetite;
- Those who have endocrine system disorders, gastrointestinal diseases;
- Women who use hormonal drugs, including contraceptives;
- People who take psychotropic drugs.
Doctors recommend following some recommendations to prevent weight gain:
- Eat food in small portions, chewing it well;
- Timely treat pathologies of internal organs and systems;
- Lead a healthy lifestyle, including physical activity;
- Avoid stressful situations, depression, emotional stress.
These rules are not difficult to follow, but they will help reduce the risk of obesity.
Treatment
If a patient is diagnosed with stage 1 nutritional obesity, the disease can be managed at home and the development of hypertension, liver and joint pathologies can be prevented. To get rid of excess fat deposits, treatment tactics are used, which include a number of measures. A treatment regimen is proposed containing:
- the first stage is dietary nutrition;
- regular physical activity;
- medications;
- correction of the usual lifestyle;
- folk remedies for weight loss;
- massage.
Normalization of nutrition is one of the important components of the treatment of patients with stage 1 obesity. There are the following diet rules:
- Eating fruits and vegetables that have a low glucose content in their raw form.
- Introduction to the menu of low-calorie foods.
- Use of plant fiber.
- Limiting fatty, spicy, smoked, fried foods and spices.
- Reducing daily salt intake to four grams.
- Exclusion of products made from flour, sweets, sugar, animal fat.
- Maintaining daily caloric intake at 1200 kcal.
Experts recommend adhering to the following diet principles:
- Carry out fasting days once a week.
- Introduce split meals with snacks between main meals.
- Eat in small portions.
- Reduce the amount of fast carbohydrates in your diet.
- Drink up to 1.5 liters of water per day.
- The last meal is three hours before bedtime.
- Avoid alcohol, which stimulates appetite.
- Adjust your eating habits.
- Take multivitamins.
Drug therapy
For obesity of exogenous constitutional origin, which has the first degree, medications are prescribed in rare cases. Drug therapy is aimed at regulating appetite by influencing the satiety center of the hypothalamus. Medicines have many contraindications. The following side effects often occur:
- increased blood pressure;
- dizziness;
- hyperemia;
- insomnia;
- headache;
- anxiety;
- dry mouth;
- nausea;
- tachycardia;
- diarrhea.
Indications for drug treatment for stage 1 disease are a BMI value of more than 30 kg/m2, or data of more than 27 kg/m2 with concomitant diabetes mellitus, hyperlipidemia - high fat content in the blood. The drugs should be prescribed by an endocrinologist. These may be the following medications:
Lifestyle correction
With exogenous constitutional pathology, weight loss requires lifestyle changes. Doctors give patients instructions to normalize their psycho-emotional state, eliminate stress and negative mood. The treatment method includes the following recommendations:
- Do morning exercises every day.
- Take walks in the fresh air.
- Use physiotherapeutic procedures - ozone therapy, Charcot's shower, underwater massage.
You can quickly cope with exogenous constitutional pathology if you adhere to the following rules:
- Get aerobic exercise at least three times a week - swimming, water aerobics, on a treadmill, or an exercise bike.
- Perform a complex of therapeutic exercises.
- Cleanse your intestines regularly.
- Sleep at least 8 hours, go to bed no later than 23.
- Treat concomitant diseases - pathologies of the thyroid gland, diabetes, digestive organs.











